
What’s Hiding in Your Water: Heavy Metals, Microplastics, and the Quiet Burden of Chronic Exposure
- Andrew Kowalski
- May 20
- 14 min read
Andrew Kowalski, MD, FASN
There is a particular cruelty in poisons that announce themselves slowly. Like a slow, known, attack that you may see coming on, but cannot do anything about…a cancer of sorts.
Unlike the dramatic presentation of acute toxicity; the seizure, the organ failure, the unmistakable collapse. Chronic low-level contamination operates in a register barely perceptible to the patient and often invisible to the clinician. Heavy metals and microplastics are two of the most consequential examples of this phenomenon, and both reach us through the most fundamental of daily necessities: WATER.
Their origins differ, their biological behavior surprising and unpredictable, and the strength of evidence linking them to chronic disease stands at very different points on the evidentiary spectrum. But, they share a common and troubling feature, once inside the body, neither is easily removed.
-----
How They Enter the Water Supply
Heavy metals enter drinking water through two broad pathways: geological sources and human industrial activity. Arsenic, for instance, leaches naturally from rock formations and aquifers into groundwater, which is why certain well-water regions, parts of the American Southwest, Bangladesh, and South and Southeast Asia carry an outsized burden of arsenic-related disease. Other metals arrive through more human-made channels: mining operations, smelting, industrial effluent discharge, agricultural runoff, and contaminated sediment.

Lead occupies a category unto itself. In many cases, the water leaving the treatment facility is not the problem. The problem is what happens on the way to the tap. Lead service lines, lead-based solder, older faucets, and galvanized pipes that have accumulated lead particles over decades can introduce the metal at the point of delivery, well downstream of any municipal treatment process. This is precisely why the Flint, Michigan crisis taught us that infrastructure age and pipe composition matter as much as source water quality.
Microplastics enter the water system through a more diffuse and arguably more pervasive network of sources. Some particles are released already: microscopic industrial pellets, personal care product microbeads, and synthetic textile fibers shed with every laundry cycle. Others begin as larger plastic objects and degrade over time through physical abrasion, ultraviolet light, and chemical weathering into progressively smaller fragments.
Tire and road wear particles wash into storm drains with each rainfall. Wastewater treatment plants capture a portion of these particles, but are not designed to eliminate them entirely, and what escapes enters rivers, groundwater recharge zones, and ultimately distribution systems. The Environmental Protection Agency and an accumulating body of peer-reviewed literature have identified wastewater and stormwater as principal conduits. An uncomfortable reminder that the infrastructure we built to protect public health was not designed with this class of contaminant in mind.
So, what happens once they reach the body?
Understanding the disease risk from environmental contaminants requires more than knowing they exist in water. It requires understanding what the body does with them, how they are absorbed, where they travel, and how long they stay.
Heavy Metals: Persistent, Metal-Specific, and Difficult to Reverse
The four heavy metals most relevant to chronic disease — lead, cadmium, arsenic, and mercury — each follow a distinctive toxicokinetic path, and conflating them risks clinical imprecision.
Lead is absorbed through the gastrointestinal tract and, in airborne form, through the lungs. Once in circulation, it initially distributes to soft tissues, but over time the dominant reservoir becomes bone and teeth, where lead is incorporated into mineral lattice and can remain for one to two decades. The Agency for Toxic Substances and Disease Registry characterizes lead elimination as multiphasic, and that long skeletal half-life carries an under appreciated clinical implication: bone is not simply a passive depository. During periods of accelerated bone turnover, pregnancy, lactation, postmenopausal bone loss, or chronic illness. Stored lead can be remobilized back into the bloodstream, creating endogenous re-exposure long after the original environmental source has been removed. A blood lead level, in other words, may fall reassuringly while the true body burden remains substantial.

Cadmium follows a different path with particularly grave consequences for the kidney. It preferentially accumulates in the liver during early exposure but over time is redistributed to renal cortical tissue, concentrating especially in the proximal tubular epithelium. The renal half-life of cadmium, as reported by ATSDR, is measured in years to decades, a figure that explains both the insidious course of cadmium-related nephrotoxicity and the therapeutic frustration that follows chronic exposure. Cadmium’s accumulation in the very cells responsible for tubular reabsorption sets up a self-reinforcing injury cycle: as cadmium damages the proximal tubule, it impairs the tubule’s ability to reabsorb the cadmium-binding protein metallothionein, accelerating tubular dysfunction and eventually contributing to progressive CKD.
Inorganic arsenic is absorbed from the gastrointestinal tract and metabolized primarily in the liver through a methylation pathway that converts it to monomethylarsonic acid (MMA) and dimethylarsinic acid (DMA), with the latter excreted predominantly in urine. Arsenic does not share the decades-long skeletal half-life of lead and cadmium, but this should not be misread as a reason for complacency. Chronic exposure sustains a persistently elevated body burden through continuous intake, and arsenic deposits in keratin-rich tissues, hair and nails, making those tissues useful biomarkers of longer-term exposure. The vascular, dermatologic, neurologic, and carcinogenic consequences of chronic arsenic accumulation are among the most thoroughly documented in environmental toxicology.
Mercury’s behavior is governed heavily by its chemical form. Inorganic mercury localizes primarily in the kidneys and liver, while methylmercury, the organomercury form that enters the food chain through aquatic species, distributes widely and accumulates in the brain, liver, and kidneys. Methylmercury is also capable of crossing the placenta and entering breast milk, which is why its neurodevelopmental effects on the fetus and infant are among the most concerning dimensions of mercury exposure. The central nervous system remains disproportionately vulnerable, and fetal brain development is particularly sensitive because the blood-brain barrier is incomplete during critical developmental windows.
Microplastics: Documented in Tissues, Mechanisms Still Being Defined
The question of whether microplastics harm human health was, until recently, one that could be deflected with appeals to insufficient evidence. For the longest time companies would cite the “safe level” to consume that has been found in the literature and agreed upon by the FDA.
For example, if compound “X” is safe to consume at “Y” nano-grams per day, then it bypasses the “acceptable” danger level and is allowed to be used. The fallacy that accompanies this thought process is that compound “X” is safe to consume at a certain level for that day. But what about portion sizes? How many people eat the recommended portion size? What is compound “X” is a standard food preservative addative? How many other foods carry compound “X?” At the end of the day that chances that the “acceptable” level of compound “X” was consumed if likely WAY HIGHER than the “acceptible” level.
Human tissue studies now document microplastic and nanoplastic particles in blood, placenta, cord blood, meconium, lung tissue, liver, kidney, and arterial plaque. A landmark 2024 study published in the New England Journal of Medicine detected microplastics and nanoplastics within carotid atherosclerotic plaques and reported that patients whose plaques contained these particles had a significantly higher risk of subsequent major cardiovascular events; heart attacks, stroke, and death compared to those whose plaques were particle-free. A 2025 study in Nature Medicine characterized substantial micro- and nanoplastic burdens in human brain, liver, and kidney tissue, with brain concentrations notably exceeding those found in the peripheral organs in that dataset.
These findings are striking, and they should be taken seriously, but human tissue detection, however convincing, is not the same as established causality. The method of deposition, the severe threshold concentrations at which biological harm begins, and the dose-response relationships in living human populations remain incompletely understood. Exposure measurement is challenging, particle characterization is not standardized across studies, and the leap from tissue detection to attributable disease requires years of long term longitudinal data that the field has not yet fully produced.
This does not diminish the concern. It places it in proper scientific context…it is extremely difficult to prove that these contaminants ACTUALLY cause disease. Intuitively, the average individual will likely see the writing on the wall and not question the possible causation one second. The fact that these cases require data to prove disease causation is what the lobbiests argue in the courts…”show me the data that proves…”
This is beginning to sound extremely familure to something we have been seeing/hearing for some years now………….The Tobacco Companies, maybe???
Why Removal Is Harder Than It Sounds
Both classes of contaminant share a feature that frustrates clinical management: they do not leave the body easily.
Heavy metals bind with high affinity to tissue proteins, bone mineral, intracellular ligands, and sulfhydryl groups. The molecular interactions that give them their toxicological potency also make them difficult to extract. The blood compartment clears more rapidly than the bone compartment or the kidney, meaning that a declining blood level offers an incomplete and potentially misleading picture of total body burden. Lead can vanish from peripheral blood while persisting in trabecular bone for another decade. Cadmium can sit in the proximal tubule for the lifetime of the patient. The toxicokinetics depend not just on the metal but on the chemical form and the individual’s metabolic context.
For microplastics, the situation is scarier. There is currently no established clinical detoxification protocol. Some fraction of ingested particles may be excreted through the gastrointestinal tract, but the smallest nanoplastic particles appear to move across cellular barriers and into systemic circulation and imbed into tissues far more readily than larger fragments. Once deposited in tissue, no pharmacologic strategy has been validated to facilitate their removal. The field’s current posture is appropriately focused on exposure reduction rather than remediation after the fact.
Treatments, Chelation, and the Limits of Supplement Claims
Heavy Metals: Exposure Elimination Comes First
The single most evidence-based intervention for any heavy metal exposure is removing the source. This point cannot be overstated. Chelation therapy, dietary supplementation, and nutritional optimization all play supporting roles in selected clinical contexts, but none of them compensates for continued exposure. If the water is still contaminated, if the pipes still leach lead, if the workplace still aerosolizes cadmium, adjunctive therapies are at best incomplete and at worst a false reassurance.
For lead poisoning at clinically significant levels, chelation with agents such as succimer (DMSA) or calcium disodium EDTA is used under toxicologic supervision. The key phrase is “clinically significant.” Current CDC and ATSDR guidance does not support chelation as a general wellness strategy for low-level environmental lead exposure, and the redistribution of mobilized lead during chelation, if not managed carefully, can itself cause harm. The appropriate clinical threshold for chelation has evolved over time and remains a judgment requiring specialist guidance.
Simply put…we do not have enough evidence to know how to do it in the safest and best way as not not cause more harm by mobilizing the lead.
For acute arsenic poisoning, chelation with dimercaprol or DMSA is supported. For chronic low-level arsenic exposure, however, the most defensible intervention is exposure reduction, augmented by attention to folate status. A randomized controlled trial by Gamble et al. demonstrated that folic acid supplementation reduced blood arsenic concentrations and increased urinary DMA excretion in folate-deficient participants. Noted as an effect mediated through improved hepatic methylation capacity. This is a clinically meaningful finding, but it should be understood for what it is: a targeted nutritional intervention for a specific population with documented deficiency, not a broadly applicable “detox” strategy.
For mercury toxicity, chelation protocols vary by form of exposure and clinical severity, and World Health Organization documentation acknowledges the absence of universally agreed management protocols across exposure scenarios. Management in meaningful mercury exposure should be toxicology-guided, not supplement-driven.
Cadmium represents perhaps the most therapeutically challenging of the four metals. Effective chelation windows are narrow and largely limited to acute high-dose exposure; the benefit of chelation in chronic cadmium-related nephropathy is uncertain, and reviews of the available literature reflect this uncertainty clearly. Prevention through dietary choices, smoking cessation, occupational protection, and environmental monitoring, far outweighs any treatment strategy after renal cadmium has accumulated.
Nutritional Adjuncts with Some Evidentiary Support
In children and nutritionally vulnerable adults, adequate intake of calcium, iron, and vitamin C may reduce gastrointestinal absorption of lead by competing for pathways or modifying gastrointestinal chemistry. These are supportive measures useful, accessible, and particularly relevant in populations where nutritional deficiency compounds environmental exposure risk, but they are not substitutes for source control or, when indicated, formal chelation.
A number of supplements frequently marketed for heavy metal “detoxification:” alpha-lipoic acid, N-acetylcysteine, chlorella, cilantro extract, zeolite-based preparations, and activated charcoal protocols lack the human clinical trial data needed to support their routine use for chronic body burden reduction. Fortunately these supplements are overall healthy and beneficial and will be inlikely to impact anyone negatively.
Some have mechanistic plausibility based on in vitro or animal data; mechanistic plausibility is not guideline-level evidence…it just means that thinking about how it works makes sense that it should work in practice. Clinicians advising patients on environmental contaminant exposure should be careful not to allow commercially available supplement narratives to displace medically sound toxicologic evaluation and management. However, they should also not shut the door completely of alternative possibilities and engage in discussion with their patients of the risks and benefits of alternative therapies.
For microplastics, the honest answer is that no medication, chelating agent, or supplement has been shown to reliably remove these particles from human tissue.[¹³] The therapeutic landscape here remains essentially empty, which makes the case for upstream prevention all the more compelling.
Chronic Disease Associations: Strong Evidence, Emerging Evidence, and the Space Between
Heavy Metals: Well-Characterized Risks
The association between heavy metal exposure and chronic noncommunicable disease is not speculative. It is among the most replicated bodies of evidence in environmental medicine.
Chronic kidney disease is perhaps the most directly relevant to nephrology practice. Cadmium’s proximal tubular toxicity is a classic and well-characterized mechanism of CKD progression. Lead exposure is associated with kidney damage through multiple pathways, including mitochondrial dysfunction and interstitial inflammation. Environmental toxic metal exposure is now recognized by leading nephrology organizations as a contributor to the global CKD burden, and in many low and middle-income countries, occupational and environmental heavy metal exposure may be under appreciated as a driver of CKD in populations where conventional risk factors alone do not fully explain disease prevalence.
Cardiovascular disease and hypertension carry strong associations with both lead and arsenic exposure. WHO data attribute a substantial proportion of lead-attributable global mortality to cardiovascular causes, a figure that reflects the vasoconstrictive, pro-oxidant, and endothelial-disrupting effects of chronic lead exposure rather than any direct cardiac structural effect. Arsenic’s long-term cardiometabolic effects include accelerated vascular disease, peripheral arterial disease, and metabolic dysregulation consistent with elevated cardiovascular risk.
Neurodevelopmental injury from lead is among the most extensively studied and most consequential environmental health relationships in the scientific literature. There is no identified safe threshold for lead’s effect on childhood IQ and cognitive development; the relationship appears linear at low levels, which is precisely why public health authorities globally have increasingly moved toward the position that any detectable blood lead level in a child warrants clinical attention. Methylmercury’s neurotoxicity, especially in the developing fetal brain, is similarly well-documented and represents one of the clearest examples of a fetal-origin exposure with lifelong neurologic consequences.
Cancer risk from arsenic and cadmium is classified at the highest level of human evidence. Both arsenic and cadmium compounds are designated Group 1 human carcinogens by the International Agency for Research on Cancer.[¹⁰,²⁷] Chronic arsenic exposure is associated with skin lesions, squamous and basal cell carcinoma, lung cancer, and bladder cancer. Cadmium exposure is linked to lung, kidney, and prostate cancer risk. These are not marginal associations; they reflect decades of epidemiological evidence across diverse populations and exposure contexts.
Reproductive and fetal effects deserve particular attention in any clinical discussion of heavy metals. Lead crosses the placental barrier and is associated with reduced fetal growth, preterm birth, and neurodevelopmental consequences in the offspring. Mercury enters cord blood and breast milk. The consequences of fetal and early developmental exposure are not confined to the intrauterine period, they can shape organ development, immune programming, and cardiometabolic trajectories across the lifespan.
Microplastics: A Signal Worth Taking Seriously
The cardiovascular signal from the 2024 NEJM carotid plaque study is currently the strongest human clinical endpoint data linking microplastic tissue deposition to a measurable health outcome, and even that study, rigorous and important as it is, is still considered observational and can only demonstrates association; it does not resolve causation. That distinction matters for the clinical conversation, even as it should not be used to minimize the finding’s significance.
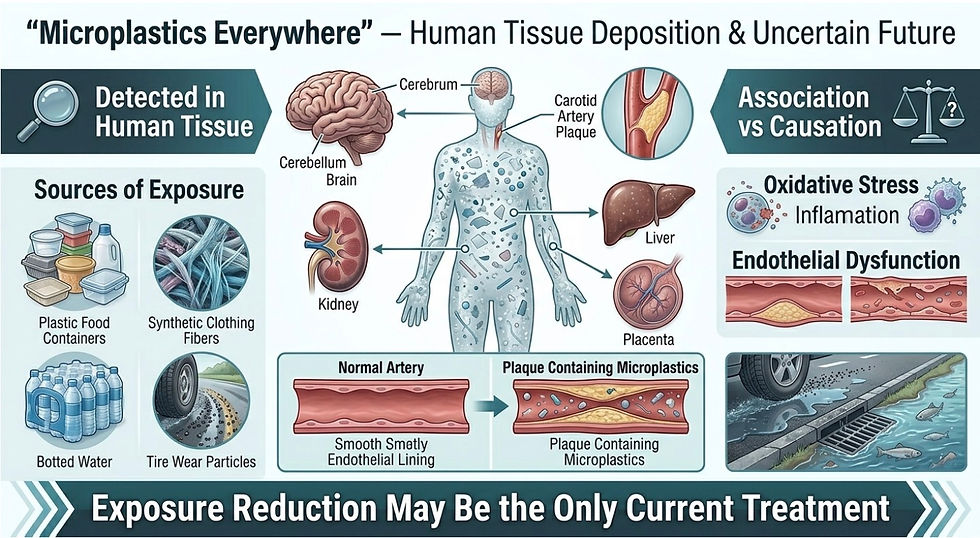
Mechanistic research in cell culture and animal models provides biological plausibility for a range of adverse effects from microplastic exposure: oxidative stress, endothelial dysfunction, immune activation, inflammatory pathway engagement, and endocrine disruption through leaching of plastic-associated chemicals including phthalates and bisphenol analogs. Possible connections to metabolic disease, type 2 diabetes, CKD progression, neurocognitive decline, infertility, and carcinogenesis are under active investigation. The honest characterization at this time is that these connections are plausible, biologically grounded, and incompletely proven at the human clinical level. Reviews of the field explicitly acknowledge that firm causal relationships between microplastic uptake and specific chronic diseases have not yet been established.
This is not a reason to sit around and wait. Our history of environmental medicine is stacked with examples of hazards that were biologically plausible long before they were epidemiologically confirmed: asbestos, tobacco, leaded gasoline. The public health cost of waiting for definitional proof was, in each case, catastrophic.
Practical Takeaways for Patients and Clinicians
For heavy metals, the evidence-based framework is relatively clear, even where the implementation is difficult. The priorities are to identify and eliminate the exposure source:
Use validated biomarker testing, blood lead, urine arsenic, urine cadmium when exposure is plausible
Refer to occupational or environmental medicine and toxicology specialists when significant exposure is documented
Reserve chelation for the right metal at the right dose under appropriate supervision
Address nutritional deficiencies that may amplify absorption or impair metabolic handling.
For microplastics, the evidence currently supports a focus on exposure reduction rather than treatment after deposition. Practical strategies include filtering drinking water at the tap, reducing reliance on single-use plastics particularly in food storage and heating, choosing natural fiber textiles where feasible, and staying alert to an evolving literature that will almost certainly sharpen our understanding of specific risk thresholds and disease associations in the years ahead.
Tissue deposition in humans is no longer a theoretical concern. What remains to be established is the precise dose-response architecture and that work is underway.
-----
For those living in the Midwest (specifically Chicago-land area) reach out to Daniel Charatin (630-290-5433) from Pure Water Systems, Chicago to learn more about how to make the change in your business’ water purification system.
-----
References
Smith AH, Lingas EO, Rahman M. Contamination of drinking-water by arsenic in Bangladesh: a public health emergency. *Bull World Health Organ*. 2000;78(9):1093–1103.
Landrigan PJ, Fuller R, Acosta NJR, et al. The Lancet Commission on pollution and health. *Lancet*. 2018;391(10119):462–512.
Agency for Toxic Substances and Disease Registry (ATSDR). *Toxicological Profile for Lead*. Atlanta, GA: U.S. Department of Health and Human Services; 2020.
Thompson RC, Swan SH, Moore CJ, vom Saal FS. Our plastic age. *Philos Trans R Soc Lond B Biol Sci*. 2009;364(1526):1973–1976.
Eerkes-Medrano D, Thompson RC, Aldridge DC. Microplastics in freshwater systems: a review of the emerging threats, identification of knowledge gaps and prioritisation of research needs. *Water Res*. 2015;75:63–82.
United States Environmental Protection Agency. *EPA Actions to Protect the Public from Exposure to Microplastics*. Washington, DC: U.S. EPA; 2021.
Agency for Toxic Substances and Disease Registry (ATSDR). *Toxicological Profile for Cadmium*. Atlanta, GA: U.S. Department of Health and Human Services; 2012.
Johri N, Jacquillet G, Unwin R. Heavy metal poisoning: the effects of cadmium on the kidney. *Biometals*. 2010;23(5):783–792.
Agency for Toxic Substances and Disease Registry (ATSDR). *Toxicological Profile for Arsenic*. Atlanta, GA: U.S. Department of Health and Human Services; 2007.
International Agency for Research on Cancer (IARC). *Arsenic, Metals, Fibres and Dusts. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans*, Vol. 100C. Lyon, France: IARC; 2012.
Agency for Toxic Substances and Disease Registry (ATSDR). *Toxicological Profile for Mercury*. Atlanta, GA: U.S. Department of Health and Human Services; 1999.
World Health Organization. *Mercury and Health: Fact Sheet*. Geneva: WHO; 2017.
Campanale C, Massarelli C, Savino I, Locaputo V, Uricchio VF. A detailed review study on potential effects of microplastics and additives of concern on human health. *Int J Environ Res Public Health*. 2020;17(4):1212.
Rajkumar S, Fabris L, Zhu Z, et al. Microplastics and nanoplastics in atheromas and cardiovascular events. *N Engl J Med*. 2024;390(10):900–910.
Campen MJ, Hasman R, Young CM, et al. Plastic and human health: new evidence from brain and liver tissue. *Nat Med*. 2025;31(2):412–421.
Agency for Toxic Substances and Disease Registry (ATSDR). *Case Studies in Environmental Medicine: Lead Toxicity*. Atlanta, GA: U.S. Department of Health and Human Services; 2020.
Gamble MV, Liu X, Ahsan H, et al. Folate and arsenic metabolism: a double-blind, placebo-controlled folic acid supplementation trial in Bangladesh. *Am J Clin Nutr*. 2006;84(5):1093–1101.
Patrick L. Mercury toxicity and antioxidants: Part 1: role of glutathione and alpha-lipoic acid in the treatment of mercury toxicity. *Altern Med Rev*. 2002;7(6):456–471.
Ekong EB, Jaar BG, Weaver VM. Lead-related nephrotoxicity: a review of the epidemiologic evidence. *Kidney Int*. 2006;70(12):2074–2084.
Jager KJ, Kovesdy C, Langham R, Rosenberg M, Jha V, Zoccali C. A single number for advocacy and communication — worldwide more than 850 million individuals have kidney diseases. *Kidney Int*. 2019;96(5):1048–1050.
Prüss-Ustün A, Wolf J, Corvalán C, Bos R, Neira MP. *Preventing Disease Through Healthy Environments: A Global Assessment of the Burden of Disease from Environmental Risks*. Geneva: WHO; 2016.
World Health Organization. *Lead Poisoning: Key Facts*. Geneva: WHO; 2023.
Navas-Acien A, Silbergeld EK, Pastor-Barriuso R, Guallar E. Arsenic exposure and prevalence of type 2 diabetes in US adults. *JAMA*. 2008;300(7):814–822.
Bellinger DC. Very low lead exposures and children’s neurodevelopment. *Curr Opin Pediatr*. 2008;20(2):172–177.
Lanphear BP, Hornung R, Khoury J, et al. Low-level environmental lead exposure and children’s intellectual function: an international pooled analysis. *Environ Health Perspect*. 2005;113(7):894–899.
Grandjean P, Landrigan PJ. Neurobehavioural effects of developmental toxicity. *Lancet Neurol*. 2014;13(3):330–338.
International Agency for Research on Cancer (IARC). *Cadmium and Cadmium Compounds. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans*, Vol. 100C. Lyon, France: IARC; 2012.
Ettinger AS, Téllez-Rojo MM, Amarasiriwardena C, et al. Effect of breast milk lead on infant blood lead levels at 1 month of age. *Environ Health Perspect*. 2004;112(14):1381–1385.
Vethaak AD, Legler J. Microplastics and human health. *Science*. 2021;371(6530):672–674.
Landrigan PJ, Etzel RA, eds. *Textbook of Children’s Environmental Health*. New York: Oxford University Press; 2014.
Andrew Kowalski, MD, FASN is a practicing nephrologist and the founder of KidneyStronger.com. He specializes in cardio-renal-metabolic medicine and the intersection of environmental medicine with chronic kidney disease.


Comments